On Monday, the U.S. Supreme Court sided with parents and reinstated an earlier federal district court ruling which blocked enforcement of California policies allowing schools to socially transition children (the use of cross-sex names and pronouns) without parental input. Despite the earlier court ruling, the 9th Circuit Court of Appeals put that order on hold, prompting an appeal to the Supreme Court. In the mixed ruling–the court sided with parents although turned down the challenge from teacher co-plaintiffs–the majority determined that the parents were likely to prevail on the merits of their claim that the California policies interfered with their due process rights under the 14th amendment, and their right to the free exercise of religion under the 1st amendment. For these reasons, the court determined that the policies are subject to “strict scrutiny” and that the California policies would not pass the legal test because they “cut out the primary protectors of children’s best interests: their parents.”
On Tuesday, the Administration for Children and Families (ACF) sent a letter to all fifty states reinforcing the notion that state agencies can only base child removal decisions on objective evidence of abuse or imminent risk of harm, and not simply because a parent declines to support a child’s cross-sex identity. The letter also warns state agencies that removing children from parents based solely on the parent’s moral convictions or religious beliefs raises constitutional concerns. “When states overstep their bounds, ACF will take action to deter inappropriate policies that drive unnecessary interactions with child welfare systems. This is one such example,” said Assistant Secretary Alex J. Adams.
Texas Attorney General Ken Paxton has issued a legal opinion that expands the scope of SB14–Texas’ law prohibiting health care providers from rendering medical transition procedures to minor patients–to mental health care providers licensed by the state’s Behavioral Health Executive Council. The opinion asserts that because the council’s licensees are considered health care providers under state law, the legislature’s prohibition against “unlawfully transitioning kids” extends to mental health professionals licensed by the state. “Any licensee that facilitates the provision of unlawful procedures or treatments that aim to transition a child’s sex are thus forbidden from receiving public money in support of those efforts and, separately, risk revocation of their licenses to practice” the opinion states.
In the wake of NYU Langone’s decision to suspend pediatric medical transition procedures, New York Attorney General Letitia James has sent a letter to the hospital suggesting that it is running afoul of state anti-discrimination law, and ordering it to resume treatment. Last month, NYU Langone announced that changes to the “regulatory environment”—presumably, anticipation of two Trump administration proposed federal rules—necessitated ending “affirming care” interventions for patients under 19. The AG’s office has given the hospital until 3/11/26 to comply, although it remains unclear what action the office will take.
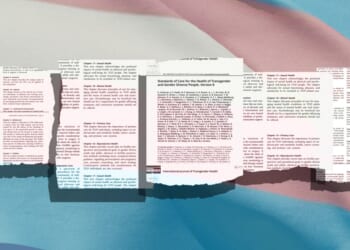
A new peer-reviewed paper in the Archives of Sexual Behavior concludes that WPATH’s clinical practice guidelines, the SOC-8, have significant limitations including a lack of rigor in development, compromised editorial independence, and clinical inapplicability. The study aimed to understand the guidelines from the perspective of health professionals, and the study recruited six clinicians and two guideline methodologists to assess key chapters of the SOC-8 using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument. Ultimately, the mean quality score for each chapter was a 3.5 to 4 out of 7, and three assessors outright recommended not using the guidelines. “We call for concerted efforts to create high-quality, evidence-based guidelines that better serve the healthcare needs of trans-identified children and adolescents. Moreover, our findings underscore the importance of enhancing the applicability of guideline recommendations in future development and adoption processes” the authors conclude.
Dovetailing with this, I wrote for the Dispatch about the history and significance of WPATH’s clinical practice guidelines, the Standards of Care, and explain their relevance for future malpractice litigation. I also go on to argue how ideological tenets baked into the guidelines–the immutability of cross-sex identities, the embrace of the “gender incongruence” paradigm, and the adoption of “minority stress theory”–undermine its simultaneous recommendations for proper assessment and “differential diagnosis.” Not surprisingly, the “affirmative care” model’s emphasis on affirmation ensures that the clinical decision-making tree typically ends in medical affirmation.
In the Wall Street Journal, Laura Hanford Bryant and Erin Friday contextualize the significance of Sage Blair attending the recent State of the Union address. Blair’s harrowing story–she was repeatedly sex-trafficked and sexually assaulted–after being separated from her legal guardians over abuse claims related to “misgendering” exposes the ways in which “abuse” has been overinterpreted to infringe on parental rights. “The child-welfare system has been hijacked through federally and state-funded programs to classify parents as abusive if they don’t accept their children’s assertions that they are members of the opposite sex. Several liberal states have codified this view into law” Friday and Hanford Bryant go on to explain. For many readers, Blair’s story is likely a wakeup call that reveals how the child-welfare infrastructure paradoxically ends up harming the very same children it was meant to protect.
As the UK’s planned clinical trial of puberty blockers for the treatment of dysphoria is put on hold, psychiatrists are urging the UK government to do a follow-up, data-linkage study of the roughly 9,000 minors who sought care at the now shuttered Tavistock clinic. “There will be a lot we can learn from this cohort [of ex-Tavistock patients] and this should now be the priority…It was alarming to learn that National Health Service adult clinics refused to co-operate with the research team who were tasked with this follow-up study, and we would hope that a reinvigorated effort would now be undertaken.” To these psychiatrists, a follow-study of youth who already received these interventions–given their risks–is more ethical than exposing another patient cohort.
Joseph Figliolia
Policy Analyst