Authored by Kimberly Drake via The Epoch Times (emphasis ours),
What do hot flashes, back pain, and insomnia have in common? Increasingly, they all lead to the same prescription: gabapentin.

The anti-seizure medication has quietly become the fifth most prescribed drug in the U.S., not because seizure disorders are skyrocketing, but because doctors are writing millions of prescriptions for uses the FDA never approved.
Now, as concerns mount about dependency and long-term cognitive risks, experts are questioning whether the medication warrants closer scrutiny.
Gabapentin Prescriptions Skyrocket
Gabapentin is FDA-approved to treat two conditions—partial seizures and pain occurring with a shingles outbreak (postherpetic neuralgia). Gabapentin enacarbil (Horizant), an extended-release version of the drug, was FDA approved in 2011 for treating moderate-to-severe restless legs syndrome in adults. However, gabapentin is widely prescribed for off-label indications—everything from hot flashes to back pain.
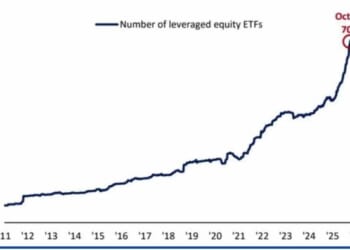
The drug’s off-label use was recently scrutinized by researchers at the CDC in Atlanta. A study published in the Annals of Internal Medicine found that the rate of gabapentin dispensing approximately doubled from 2010 to 2016 and also increased from 2016 to 2024, though at a slower rate.
Gabapentin dispensing was highest and continues to increase among older adults, which, the researchers note, may be due to the rise in off label prescribing for unexplained pain and other conditions common among people 65 years or older.
The CDC researchers noted that the drug may rank even higher on the most prescribed list, as the data used in the study did not include prescriptions dispensed outside of retail pharmacies, such as hospitals, long-term care facilities, and mail-order pharmacies.
When Gabapentin May Help
The top reason people take gabapentin is pain, especially back pain, said Erika Gray, a pharmacist, and founder and chief medical officer at ToolBox Genomics, who was not involved in the study.
“The second symptom is difficulty sleeping,” she said.
Roger Passow, a retired business owner in Wisconsin, experienced severe leg pain and weakness that disrupted his sleep and ability to walk. After X-rays revealed nothing conclusive, his doctor admitted he was “stumped.” An orthopedic specialist told Passow he would “just have to live with it.”
Without a diagnosis, a pain specialist prescribed 600 mg of gabapentin nightly. When that didn’t help much, Passow increased to 900 mg. “Even with the pills, some nights I still have pain. Almost all night. It can really be miserable,” he told The Epoch Times. Despite concerns about long-term effects, he continues taking it because he feels there’s no other option.
Evidence suggests that gabapentin may be effective for specific off-label conditions. However, in some cases, other drugs offer better benefits.
Gabapentin may help:
- Diabetes-Related Nerve Damage: Gabapentin can help reduce diabetic peripheral neuropathy pain, according to a 2025 study, but not as well as pregabalin (Lyrica) and duloxetine (Cymbalta).
- Nerve-Related Pain: A 2025 systematic review of research found that while gabapentin can reduce nerve pain, pregabalin was significantly more effective.
- Chronic Cough with Unknown Cause): A 2023 analysis of six studies including 536 participants found that gabapentin is effective for treating chronic refractory cough, and it may be safer than other similar drugs.
- Alcohol Use Disorder: Whether taking gabapentin can help people quit drinking alcohol is unclear. However, some research has shown that compared to a placebo, gabapentin can lower the number of days a person engages in heavy drinking by 18 percent.
- Hot Flashes: A 2020 meta-analysis found that women who took gabapentin reported shorter and less frequent hot flashes. The researchers suggest that it may be an alternative for women who cannot or do not want to take hormone replacement therapy.
In contrast, gabapentin may not be the best choice for people with bipolar disorder and insomnia. A 2021 systematic review published in Molecular Psychiatry found minimal evidence that the drug is effective for these two conditions.
Overall, doctors should consider trying non-drug treatments, like physical therapy, and addressing sleep problems, inflammation, or other individual factors that might be contributing to a person’s symptoms before prescribing gabapentin, Dr. Luke Barr, a board-certified neurologist and the director of neurology at Deaconess Health System in Evansville, Indiana, told The Epoch Times.
How Did Off-Label Use Become So Widespread?
Understanding gabapentin’s current popularity requires looking at both its troubled past and the genuine clinical needs it addresses.
In the late 90s, Parke-Davis, a subsidiary of Warner-Lambert, the pharmaceutical company that first marketed gabapentin under the brand name Neurontin, aggressively marketed the drug for a wide range of health conditions for which it was not approved, including ADHD, pain disorders, and migraine.
According to the U.S. Department of Justice, the company also paid doctors to attend “consultant’s meetings” where physicians received a fee for attending expensive dinners or conferences involving presentations about off-label uses of Neurontin. In 2004, after a whistleblower suit, the company agreed to plead guilty and pay $430 million in fines and civil damages for its illegal and fraudulent promotion of the drug for unapproved uses.
However, the pharmaceutical scandal from two decades ago doesn’t fully explain today’s prescribing patterns. Other factors have driven the uptick in gabapentin prescriptions — some responding to legitimate medical needs, others raising questions about appropriate prescribing.
Doctors are more willing to give patients gabapentin instead of older drugs like tricyclic antidepressants because it won’t cause as many side effects, said Barr.
Additionally, doctors consider gabapentin a better option than synthetic opioids for chronic pain. People can become dependent on opioids which has led to an addiction crisis impacting millions of Americans, resulting in over 54,000 overdose deaths in 2024 alone. Many people are aware that taking opioids carries these addiction risks, so more are demanding non-opioid drug options like gabapentin.
The drug’s relatively low cost and its potential to provide benefits for some off-label conditions may also drive the increase in prescriptions. “Together these forces create a permissive environment for off-label use, sometimes without adequate monitoring,” Barr said.
One factor driving the rise in off-label gabapentin prescribing is the lack of adequate treatment options. For many people, gabapentin provides some or enough relief that they can finally resume their daily activities, said Gray.
Understanding the Risks
Less than half of people prescribed gabapentin will not notice meaningful pain relief but will likely experience side effects or adverse events, studies suggest.
In 2019, the FDA warned patients and doctors that serious breathing problems and even death have been associated with taking gabapentin with certain medications. Barr has seen patients have excessive sedation or compromised breathing after their gabapentin prescription was combined with opioids or benzodiazepines. Some people needed emergency care, he said.
“This interaction is one of the most important safety messages,” Barr noted.
Some of his older patients have experienced falls or had to stop driving because of gabapentin’s more common side effects, like dizziness. He adds that doctors sometimes use gabapentin to treat symptoms caused by other drugs, creating a vicious cycle of adding more medications rather than addressing the root cause.
According to Gray, the dosages themselves may pose health risks for some people. “One of my biggest concerns with gabapentin is how high prescribers go with the dosages, especially with older adults or patients [taking multiple medications],” Gray said. “Additionally, gabapentin is broken down by the kidneys, and as people age, their kidney function decreases.”
She said she has seen many occasions where a patient’s kidney function has dropped, yet the prescribing doctor did not adjust the patient’s dose.
The Potential for Dependence
While far fewer people get addicted to gabapentin than opioids or benzodiazepines, the risk increases for those who use other drugs or alcohol or for people who have opioid use disorder. Several states now consider the drug a Schedule V controlled substance. Schedule V drugs have a low risk for abuse and dependence but still require a prescription due to their potential to cause addiction.
“I’ve seen requests for higher doses and evidence of nonmedical use,” Barr said. He has also witnessed patients who have used high doses of gabapentin for months experience withdrawal symptoms after suddenly stopping the drug, such as insomnia, anxiety, and rarely, seizures.
The potential for a person to go through withdrawal after taking gabapentin is why doctors recommend gradually tapering off the medication to lower the risk of experiencing these unpleasant symptoms. Withdrawal symptoms can last up to 10 days, Dr. Roger Starner Jones, Jr., a board-certified emergency and addiction medicine physician and founder of Nashville Addiction Recovery, Belle Mede AMP, and Recovery Now, told The Epoch Times.
Nicotinamide Adenine Dinucleotide (NAD+) infusions have been shown to ease symptoms of withdrawal and reduce cravings in patients who are dependent on the drug, Starner Jones added.
More Gabapentin Research Needed
Older studies investigating gabapentin’s safety and effectiveness when used to treat epileptic seizures suggest it is safe, effective, and well-tolerated. A 2013 paper found no long-term safety issues when the drug was used to treat shingles-related pain.
However, new concerns have emerged after a recent investigation revealed that the drug may increase the risk of memory issues when used long-term. The observational study, published in Regional Anesthesia & Pain Medicine, found that adults under 65 who were prescribed the drug six or more times over a 10 year period for back pain had over twice the risk of dementia and mild cognitive impairment compared to those not taking the medication.
After three years of taking gabapentin, Passow finally received an MRI that revealed the actual source of his pain: severe arthritis, bulging discs, and vertebrae pinching the nerves going to the leg. He is now awaiting treatment with steroid shots to target the affected nerves. If that doesn’t work, the next steps may involve surgery.
Passow’s case illustrates a broader concern: gabapentin can become a long-term solution for patients who might benefit from other targeted treatments. For three years, he took daily medication that provided little relief when more specific interventions were available. He hopes the steroid shots will be enough to reduce his pain so he can stop taking “so many pills.”
Mrs. Passow experienced a situation similar to her husband’s when a doctor prescribed gabapentin after failing to identify the cause of her unexplained scalp pain. “I was afraid to take it. I finally did try it, but stopped right away because it didn’t help,” she said. She later discovered that simple scalp massages, not medication, eliminated the problem.
Loading recommendations…